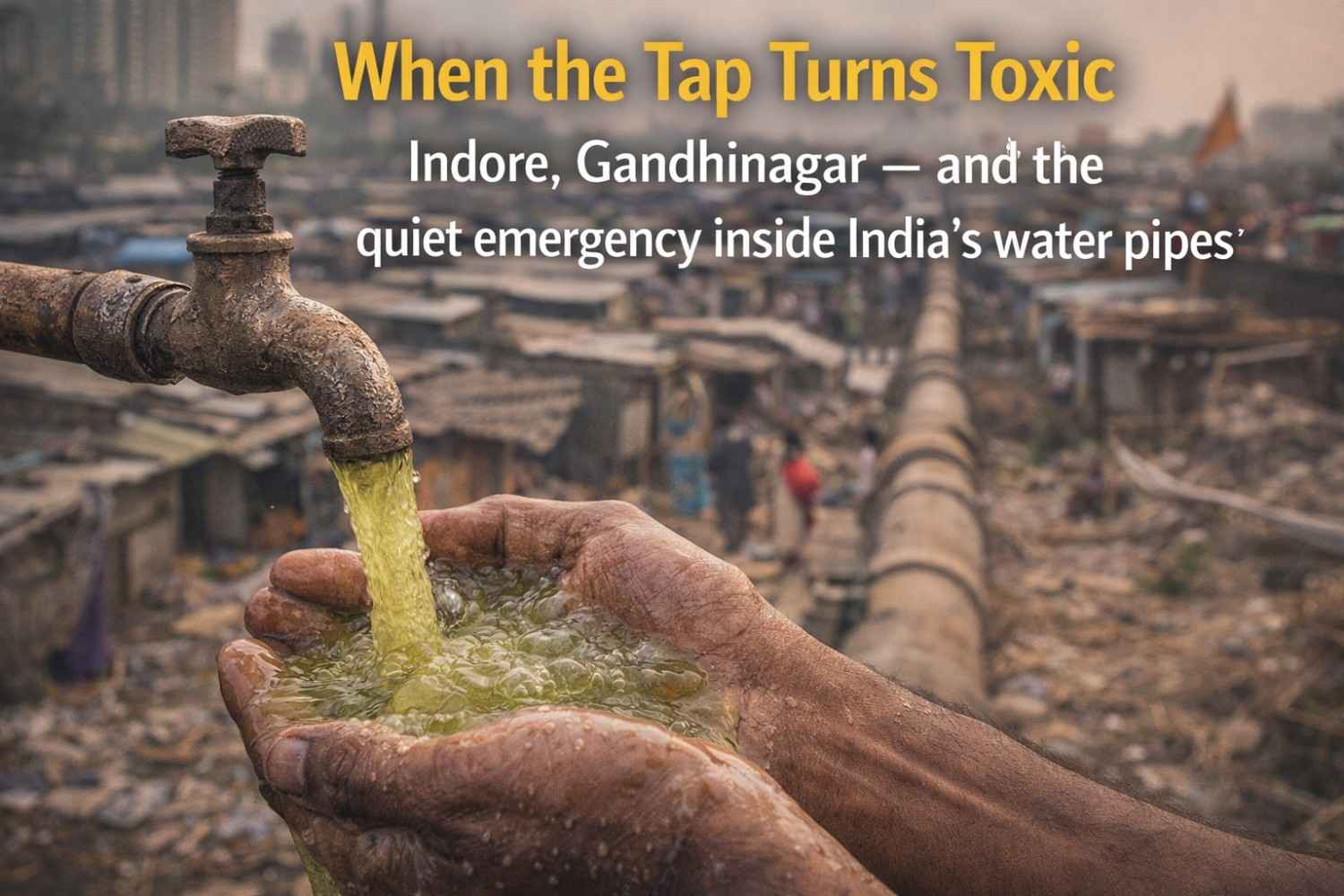
Indore, Gandhinagar — and the quiet emergency inside India’s water pipes
It began with something easy to ignore. A smell. The kind that makes you wrinkle your nose, rinse the glass again, and hope it is a one-day problem.
In Indore’s Bhagirathpura locality, Preeti Sharma says she noticed it first. The tap water, she recalls, had turned “foul-smelling”. She says she complained to the local councillor—again and again. Nothing changed. The water kept coming. So did the smell. Until the sickness arrived.
And once it arrived, it moved fast.
Families began rushing between homes, clinics, and hospital corridors with the same frightening pattern: vomiting, diarrhoea, weakness, dehydration. In a matter of days, Indore—often celebrated as India’s “cleanest city”—was confronting an uglier truth: the water itself had become a carrier of disease. Tests later confirmed bacterial contamination in drinking water, traced to leakage in the main supply pipeline.
Omprakash, another Bhagirathpura resident, showed samples of muddy tap water to reporters. “Meanwhile,” he said, “sewage kept flowing into our drinking water.” It is the kind of sentence that should never be spoken in a country that talks of smart cities and world-class infrastructure. Yet it was spoken. And people were already paying the price.
This is not only an Indore story.
In Gandhinagar, Gujarat’s capital, children began arriving at the Civil Hospital with high fever and stomach distress. In just days, over a hundred suspected typhoid cases were reported—most of them children. Doctors warned that new cases could keep emerging for the next two weeks, even as repairs and disinfection began.
Two cities. Different pathogens. One shared fear that lodges itself in the mind of every parent: what if the glass of water you gave your child was the beginning of a hospital visit?
What happened — and why it matters beyond two cities
In late December 2025 and early January 2026, contaminated drinking water triggered outbreaks of severe gastrointestinal illness in Indore and a sharp rise in suspected typhoid cases in Gandhinagar. Reports from Indore said more than 1,400 people were affected as the crisis escalated, and deaths were reported as the city struggled to contain the fallout. Gandhinagar’s hospital load was dominated by children—small bodies fighting a disease that should have been prevented long before the first fever.
These outbreaks are not random accidents. They echo a pattern public health and water-systems experts have warned about for years: leak-prone distribution lines, pressure fluctuations, ageing networks, and contamination entering water through breaks and weak points. It is not only about how water is treated at the plant. It is about what happens after treatment—inside the distribution maze that carries water to your kitchen.
Who suffers first — and who carries the burden next
Water contamination does not hit everyone equally. The first to pay are households in dense neighbourhoods and older networks—places where pipelines run close to drains, where pressure fluctuates, where “temporary fixes” become permanent risk. In Indore, residents say complaints were raised for days before the outbreak was fully recognised as a civic emergency. In Gandhinagar, too, the worst-hit were specific sectors and villages where residents reported foul-smelling, visibly dirty water.
Then comes the second burden: the hospitals.
Frontline doctors and nurses handle the overflow of dehydration cases, the panic of families, the crowding in emergency wards, and the quiet chaos of a preventable crisis. One doctor in Indore described a “deluge” of infections and warned that by the time boiling-water advisories spread widely, “it was too late” for many to avoid getting sick. For families, these are not “cases”. They are wages lost, school missed, savings drained, and fear that lingers long after the fever breaks.
When the crisis unfolds — the dangerous window nobody watches
The critical window in both outbreaks was late December 2025 through the first days of January 2026—exactly when many families were travelling, hosting relatives, or relying heavily on municipal supply during holiday routines. In Indore, the response mobilised as cases spiked around December 29–31, with outpatient attendance rising sharply in the affected locality.
This timing matters because outbreaks often become fatal when early warning signs are ignored. The smell, the colour, the turbidity, the sudden change in taste—these are not minor inconveniences. They are alarms.
Where it is happening — and why the warning lights are blinking elsewhere
Indore and Gandhinagar are the current epicentres. But the warning signs are not confined to them. Reports have also described contamination scares and pipeline-linked illness spikes in other parts of India, including areas where residents complained of frothy, foul-smelling water and suspected sewage intrusion.
Your research note underlines the wider stress signals: doubts over water quality, turbidity, faecal contamination risk, and persistent questions about monitoring transparency. When water quality data is not visible, not timely, and not trusted, the public learns the truth only after bodies start arriving at hospitals.
Why it is happening — the governance gap between knowing and doing
Water safety is not just an engineering issue. It is a governance issue.
The National Human Rights Commission took suo motu cognisance of the Indore case, citing reports that the main pipeline passed beneath a public toilet and that leakage could have allowed sewage to mix with drinking water. It also noted allegations that residents’ complaints were not acted upon.
NDTV’s reporting added a detail that should trouble every administrator: a tender to replace the Bhagirathpura pipeline had reportedly been floated months earlier, but work began only after deaths were reported.
This is the deeper failure at the heart of contaminated-water tragedies. Risks are often known. They are sometimes mapped. They can even be budgeted. But they are not fixed in time. And when time is lost, people pay in sickness, and sometimes in death.
How “clean” water becomes contaminated — the science of intrusion
Public health experts use a stark word for what happens inside damaged networks: intrusion.
Water may leave a treatment plant clean. But as it travels through cracked pipes, low-pressure stretches, or poorly maintained intersections with drainage lines, contamination can enter. It can happen through broken mains, cross-connections, and backflow during pressure drops. It can happen when sewage lines run close to drinking-water lines and a leak becomes an open doorway.
In Gandhinagar, officials traced the outbreak to sewage leakage near a drinking-water pipeline after residents complained of dirty water for nearly a week. In Indore, official confirmations also pointed to leakage and sewage mixing as likely causes. The mechanics may vary. The consequence is the same: the tap turns into a threat.
A humane truth — water is a basic service, but it is also daily trust
Municipal water is not like a road or a park. You do not simply “use” it. You put it inside your body. You give it to infants. You cook a sick parent’s meal with it. You swallow medicines with it.
So when water turns unsafe, the damage is not only medical. It is moral.
Indore’s crisis pushed that moral question into the open. When a national rights body steps in, it signals something important: safe drinking water is not a luxury. It is a duty of the state. And when that duty fails, accountability cannot be reduced to a press note or a temporary repair.
This framing matters because it changes the question. It is no longer only, “Where was the leak?” It becomes, “Why was the warning ignored?” Not only, “How did bacteria enter the line?” but “Why did the system allow delay to become disaster?”
What policymakers must do now — not in the next budget cycle
If India treats these outbreaks as “episodes”, we will keep repeating them as “seasons”. The question is no longer whether contamination can happen. It is whether we will design systems that assume it will—and prevent it before wards overflow.
The first shift must be conceptual: distribution networks must be treated as health infrastructure. Hospitals get audits. Vaccines get cold-chain monitoring. Drinking water pipelines require comparable seriousness because they are part of disease prevention, not merely service delivery. India’s drinking water standard, IS 10500, sets expectations. But standards become meaningless if the last-mile network is compromised and unmonitored.
Next, every city must be required to operate with a Water Safety Plan mindset—risk management from source to tap. Global public health guidance is unambiguous: safe water is achieved through systematic identification of risks and rapid controls, especially in distribution systems. This means mapping high-risk intersections, ensuring residual disinfection, preventing backflow, and responding quickly when pressure drops or contamination signals appear.
Then comes transparency. If residual chlorine drops in a locality, if turbidity rises, if contamination risk increases, citizens should see it as data—timely, local, and public. Not as rumours. Trust collapses in secrecy, and panic fills the gap that information should occupy.
The fourth action is procurement discipline. Indore’s reporting points to stalled work and delayed upgrades. Pipeline replacement must be treated as time-bound risk mitigation. It cannot remain a file that waits for “administrative convenience”, because bacteria does not wait for approvals.
Finally, every city needs a “first 48 hours” playbook for contamination events. Gandhinagar’s response included surveys, repairs, and disinfection steps, but such responses must become standard practice across the country: immediate alternate water supply, clear boil-water advisories, emergency chlorination, rapid sampling, and daily public updates until safety is restored.
What civil society can do — without waiting for tragedy at its own doorstep
Citizens do not run water utilities, but they can create the pressure and the early-warning systems that save lives.
It starts with recognising signals. In both Indore and Gandhinagar, residents reported foul smell, abnormal colour, and dirty water before the case numbers surged. These complaints must be treated as alerts, not inconveniences. RWAs, school committees, and ward groups can build simple reporting chains and escalation points—clear people to call, clear documentation, and collective follow-up.
Independent testing also matters. Visakhapatnam has launched a mobile water testing laboratory—a “lab-on-wheels”—to run onsite checks across wards and detect risks early. This should not remain a “good story” from one city. It should become a normal expectation everywhere.
Civil society can also support a bigger water logic: protect drinking water for drinking. Your research note highlights greywater reuse as a strong policy direction, with the potential to save 30–40% of household water by recycling domestic wastewater for non-potable purposes. Less pressure on fresh supply often means better maintenance capacity and lower risk. Water stress and contamination frequently travel together. When systems are overdrawn, maintenance weakens and risk rises.
Proof that solutions exist — if we scale what works
India does not lack solutions. It lacks speed and scale.
In Ludhiana, a canal-based water supply pipeline project is being built to improve reliable potable supply under a World Bank and AIIB-backed programme. In Chennai, Southern Railway is shifting to recycled sewage water for non-potable operations such as coach cleaning and track maintenance, reducing pressure on drinking-water resources. Your research note also points to smarter monitoring systems—AI-based tracking, predictive analytics, and real-time sensors—to detect leaks and manage networks before they turn into outbreaks.
These are not merely “innovations”. They are protections. They are public health measures in engineering form.
The bottom line — before the next glass becomes the next headline
Indore and Gandhinagar are not only news stories. They are warnings written in hospital discharge slips and, in the worst cases, in death certificates.
A country that can build metros and missions can also build water systems that do not poison the poor first. But it will require a shift in mindset—from celebrating access alone to guaranteeing safety at the tap.
Clean water is not a favour. It is a constitutional promise in practice. And in January 2026, that promise is asking India to act—before the next glass becomes the next headline.

Add a Comment